


Traditionally, a spinal curve is classified as scoliosis if it is measured above 10 degrees from a front-back view. However, scoliosis really is a spinal condition with a 3-dimensional change in the spinal alignment. When the spine is viewed from the front, it appears curved where it should be straight. The spine appears flat or has a reverse curve where it should be curved from the side view. Lastly, it appears twisted from the top down where there is normally no twist.
Traditional Medical Treatment:
Mild Scoliosis (10-25 degree curve) - Observation only
Moderate Scoliosis (26-40 degree curve) - Bracing
Severe Scoliosis (over 40 degree curve) - Surgery
What is Congenital Scoliosis?
Congenital scoliosis means the person is "born with" scoliosis. It is caused by abnormal development of one or more vertebrae from birth. However, the actual curve may not detected until later in childhood. This can be seen on X-ray. Congenital scoliosis is often associated with other problems in other areas of the body as well. Almost 25% of teens with congenital scoliosis have problems with their kidneys or urinary tract. 10% have congenital heart disease as well.
What is Idiopathic Scoliosis?
Scoliosis may be secondary to neurological disease (eg, cerebral palsy), muscular abnormalities (eg, Duchenne muscular dystrophy), spinal muscular atrophy, polio, or other syndromes (eg, Marfan Syndrome). Occasionally, significant lateral deviation of the spine can occur with little or no rotation of the spine and without bony abnormalities. In these cases, the ‘scoliosis’ can be the result of pain, spinal cord abnormalities, tumours (both intraspinal and extraspinal) and infection. The majority of scoliosis cases encountered will be without an obvious cause (idiopathic).
Adolescence Idiopathic Scoliosis (AIS) is the most common pediatric spinal deformity, affecting ~3% of children worldwide. It has no ethnic population is spared. AIS significantly impacts disability for over 10% of patients. The great majority of cases are of adolescent onset.
Common Scoliosis Braces:
The most common form of a TLSO (Thoraco-Lumbo-Sacral Orthosis) brace is called the "Boston brace," and it may be referred to as an "underarm" brace. This brace is fitted to the child's body and custom molded from plastic. It works by applying three-point pressure to the curvature to prevent its progression. It can be worn under clothing. The Boston brace is usually worn 23 hours a day, and it can be taken off to play sports, or participate in gym class during the day. This type of brace is usually prescribed for curves in the lumbar or thoraco-lumbar part of the spine.
Another type of brace is Cervico-Thoraco-Lumbo-Sacral-Orthosis brace (known as a Milwaukee brace). The Milwaukee brace is similar to the TLSO described above, but also includes a neck ring held in place by vertical bars attached to the body of the brace. It is also worn 23 hours a day, and can be taken off to play sports or participate in gym class during the day.
Charleston Bending Brace is also called a "nighttime" brace because it is only worn while sleeping. This brace is molded to the patient while they are bent to the side, and thus applies more pressure and bends the child against the curve. This pressure improves the corrective action of the brace. This type of brace is worn only at night while the child is asleep. Many studies have shown that the Charleston Night time brace is as effective as the above-described 23-hour-a-day brace wear. Curves must be in the 20 to 40 degree range and the apex of the curve needs to be below the level of the shoulder blade for the Charleston brace to be effective.
Cheneau Brace is a 3 point pressure brace that applies pressure above the curve, below the curve and at the middle of the curve. This type of brace immobilizes the patient inside it, like a cast and therefore can cause a loss of muscle strength and endurance during treatment and less of the correction is retained at the end of the treatment. Cheneau brace designs are based on the Schroth classification system of scoliosis curves.
"The New 3D ScoliBrace" The new ScoliBrace is different from all the traditional braces. ScoliBrace acheives a super corrective position by guiding the body and spine into the oppossite alignment of the scoliosis. Curve reduction can be achieved in the majority of cases as well as improvements to rib humping, shoulder levels, and the overall appearance of the body. ScoliBrace is created from 3D body scans in conjunction with x-rays and posture photos. Each brace is designed using Computer Aided Design (CAD) software and custom made.
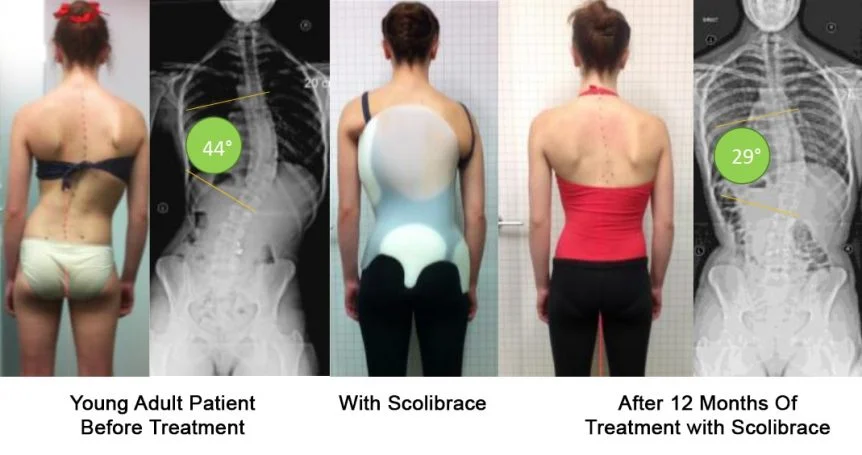
"The New 3D ScoliBrace"
The new ScoliBrace is different from all the traditional braces.
In 2013, the New England Journal of Medicine published a multi-center study to determine whether wearing scoliosis braces would prevent the need for spinal correction surgery in children with Adolescent Idiopathic Scolioisis (AIS). The study was cut short when early results were overwhelmingly in favour of bracing. This study demonstrates that when scoliosis bracing is prescribed and made properly for high-risk patients, the need for surgery can be prevented in most cases.
Long-Term effect of Surgical Option
A matched study 25 years after surgery for Adolescence Idiopathic Scoliosis revealed that there were significantly more degenerative disc changes in the lowest unfused disc in the patient group. This level also correlated to lumbar pain intensity as well as to the diminshed lumbar lordosis. The prevalence of disc aging and back pain after fusion extending into the lower lumbar spine. A matched MR study 25 years after surgery for AIS. Acta radiol 2001 Mar;42(2):187-97
Different studies have shown significant wear and corrosion in the rod. Wear was present in 75%, corrosion in 39%, and fractures in 7% of the retrieved implants according to a study in 2006. Retrieved rods exhibited corrosion, wear, and fracture, with wear and corrosion mainly located at the interfaces with hooks, screws, or crossconnectors. Wear and corrosion in retrieved thoracolumbar posterior internal fixation. Villarraga ML et al, Exponent, Inc., Philadelphia, PA 19104, USA. Spine. 2006 Oct 1;31(21):2454-62.
Another study showed corrosion on many of the rod junctions as much as 66.2% after long-term implantation. The authors recommended removal of the spinal implants after solid bony union. Corrosion of spinal implants retrieved from patients with scoliosis. Akazawa T, Minami S, Takahashi K, Kotani T, Hanawa T, Moriya H. Department of Orthopedic Surgery, Graduate School of Medicine, Chiba University, 1-8-1 Inohana, Chiba, 260-8670, Japan. J Orthop Sci. 2005;10(2):200-5.
Can leg length inequality cause scoliosis?
Leg length inequality is common, with 23% of the general population having a discrepancy of 1 cm or more. Management of Leg Length Inequality J South Orthop Assoc 10(2):73-85, 2001. © 2001 Southern Medical Association James J. McCarthy, MD, and G. Dean MacEwen, MD
It has been reported that the incidence of scoliosis is higher in patients with leg length inequality. During the growth period, 1 cm or more should be treated to prevent compensatory lumbar scoliosis.
Myth about Soliosis
It will stop getting worse once the bone growth stop.
This is a common perception about scoliosis. However, this is not the case. In one 20-year study, about 40 percent of adult scoliosis patients experienced a progression. Of those, 10 percent showed a very significant progression, while the other 30 percent experienced a very mild progression, usually of less than one degree per year.
It is a genetics disorder?
Adolescent idiopathic scoliosis probably results from a combination of genetic and environmental factors. Studies suggest that the abnormal spinal curvature may be related to hormonal problems, abnormal bone or muscle growth, nervous system abnormalities, or other factors that have not been identified. Researchers suspect that many genes are involved in adolescent idiopathic scoliosis. Some of these genes likely contribute to causing the disorder, while others play a role in determining the severity of spinal curvature and whether the curve is stable or progressive. Although many genes have been studied, few clear and consistent genetic associations with adolescent idiopathic scoliosis have been identified. A study in 2013 showed that the susceptibility gene, GPR126, is highly expressed in cartilage and that suppression of this gene leads to delayed growth and bone tissue formation in the developing spine. GPR126 is also known to play a role in human height and trunk length. (3)
All Scoliosis Patients Should Avoid
Sleeping With A light On
Melatonin is a hormone secreted by the pineal gland, a small gland deep in your brain. This hormone is responsible for many things, including the regulation of puberty in females. Melatonin is secreted primarily when you sleep, but even the smallest hint of light can slow or stop its release and create a deficiency.
Studies have confirmed a decrease in melatonin levels in patients with scoliosis. However, the reported associations are linked in pathogenesis rather than etiologic factors. Melatonin may play a role in the pathogenesis of scoliosis (neuroendocrine hypothesis) (1).
So sleeping with the lights on, the television on, a night light, a street light shining through the window, etc., is a definite no no if you have scoliosis spine. A melatonin deficiency can cause early onset pubertal growth and increase the progressive behavior of scoliosis. Quite often children that enter puberty early have an increased risk of scoliosis progression due to neurological posture immaturity, which simply means the brain and body aren’t quite in sync yet. (by Dr. Brian Dovorany)
Exercises to Avoid:
Since scoliosis is a 3-dimensional spinal deformity, certain repetitive movements can negatively influence these changes according to biomechanics concepts.
Torso Extension
Repetitive extension of the thoracic scoliosis spine should be avoided if you have scoliosis with a primary thoracic curve. The thoracic spine will be negatively impacted by the extension of this region. Biomechanically extension will cause an anterior shear force to occur which will cause the thoracic vertebrae to rotate further into the concavity of your scoliosis curve. Avoid doing backbends, gymnastics, certain yoga positions, swimming (2), and dance maneuvers that arch your body backwards.
Rotation Movement
Rotation movement may help to reduce one curve, it will likely make the opposite curve worse if the person has double curve scoliosis.
References:
1) Eur Spine J. 2011 May; 20(Suppl 1): 68–74.
2) Clin Sports Med. 1986 Jan;5(1):149-58.
3) Genetic variants in GPR126 are associated with adolescent idiopathic scoliosis. Nature Genetics, 2013; DOI: 10.1038/ng.2639
4) Toronto SickKids Hospital